This is not a scientific or technical blog about Esophageal balloons like how to insert, trouble shoot etc, but rather an argument for why using esophageal guided manometry during mechanical ventilation should not be optional or luxury or for research purposes only but should be a routine like using the information given by other ventilator graphics.
I know what you are thinking, lots of studies didn’t show mortality benefit using the esophageal balloon, and I will argue back that they said the same about the Pulmonary artery catheters, proning and lots of other examples in medicine. Having a measuring device doesn’t improve mortality, however using the information given correctly might and probably does. Lets agree to disagree.
The goal is “Individualized Mechanical Ventilation”
lets leave the curse of one hat fits all (TV 6ml/kg, Plateau < 30, DP < 15)
Argument for why we should use it?
To prevent or reduce VILI
- Trans-pulmonary pressures (inspiratory, expiratory, and driving pressure) are the stress acting on the lung itself versus the airway driving pressure that is the pressure acting on both the lungs and chest wall, and yes chest wall elastance are worse during ARDS, along many other causes)
- PEEP settings (the repeated opening and closing of alveoli, atelectrauma)
- Measurement of patient inspiratory effort (gold standard to measure Pmus, WOB, PTP) to reduce work shifting, diaphragmatic atrophy, VIDD
- Distinguishing between lung and chest mechanics
Management of Dyssynchronies (Patient-Ventilator Interactions)
We know they are harmful right ? It is the gold standard in diagnosing and probably managing dyssynchronies (to my knowledge no studies comparing managing dyssynchronies with or without a balloon and the outcomes were done?
Trans-vascular pressures
The CVP, PAWP are supposed to represent the filling pressures of the right and left heart (end diastolic pressures) respectively. They are affected by the pleural pressure don’t forget. For example the CVP is elevated at 15 mmHg, the pleural pressure at end expiration is 20 cmH2O (14.7 mmHg) so real trans-vascular pressure is actually very low at 0.3 mmHg
So why aren’t we using them?
Apart from lack of education or understanding, the unwillingness to spend extra time inserting, trouble shooting and yest sometimes getting frustrated with them
- Not available on all current ventilators: lame excuse but remember it was developed in the 70s before most ICU ventilators had graphics even, yes it is easier to have the catheter attached and graphs displayed on the ventilator but it can be connected to regular ICU monitor (need to convert mmHg to cmH2O, hard to compare to the other ventilator waveforms)
- Expensive: ok maybe you have a point there but compared to other expenses in ICU it actually is not that expensive
- No good evidence for improved outcomes: i hear you, there are some evidence not very strong but there is actually not much good research still so lets do some work. Remember they said that about prone position and steroids for ARDS right ?
- There are other options or technologies for measurements: good, we need multi-modal monitoring (look at the blog multi-modal monitoring)
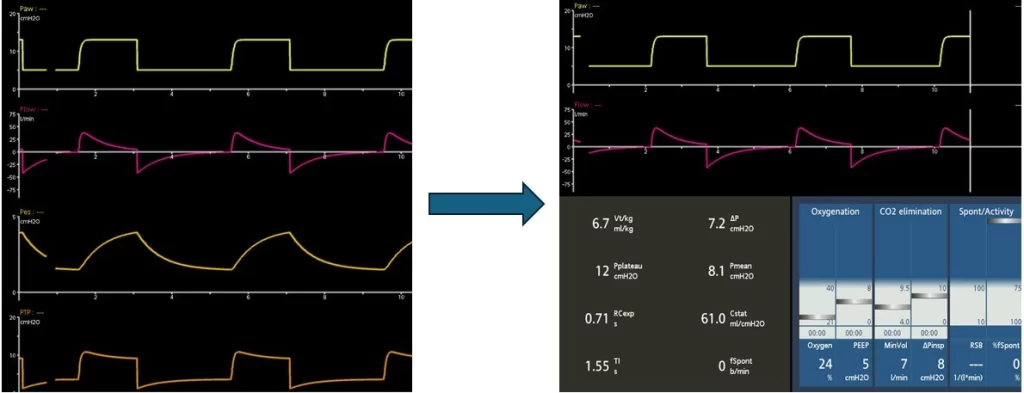
Having a problem with it or don’t want to deal with it ? No problem, Easy
Change the screen and pretend it is not there