This is not a scientific or technical blog about Esophageal balloons like how to insert, trouble shoot etc, but rather an argument for why using esophageal guided manometry during mechanical ventilation should not be optional or luxury or for research purposes only but should be a routine like using the information given by other ventilator graphics.
I know what you are thinking, lots of studies didn’t show mortality benefit using the esophageal balloon, and I will argue back that they said the same about the Pulmonary artery catheters, proning and lots of other examples in medicine. Having a measuring device doesn’t improve mortality, however using the information given correctly might and probably does. Lets agree to disagree.
The goal is “Individualized Mechanical Ventilation”
lets leave the curse of one hat fits all (TV 6ml/kg, Plateau < 30, DP < 15)
Argument for why we should use it?
To prevent or reduce VILI
- Trans-pulmonary pressures (inspiratory, expiratory, and driving pressure) are the stress acting on the lung itself versus the airway driving pressure that is the pressure acting on both the lungs and chest wall, and yes chest wall elastance are worse during ARDS, along many other causes)
- PEEP settings (the repeated opening and closing of alveoli, atelectrauma)
- Measurement of patient inspiratory effort (gold standard to measure Pmus, WOB, PTP) to reduce work shifting, diaphragmatic atrophy, VIDD
- Distinguishing between lung and chest mechanics
Management of Dyssynchronies (Patient-Ventilator Interactions)
We know they are harmful right ? It is the gold standard in diagnosing and probably managing dyssynchronies (to my knowledge no studies comparing managing dyssynchronies with or without a balloon and the outcomes were done?
Trans-vascular pressures
The CVP, PAWP are supposed to represent the filling pressures of the right and left heart (end diastolic pressures) respectively. They are affected by the pleural pressure don’t forget. For example the CVP is elevated at 15 mmHg, the pleural pressure at end expiration is 20 cmH2O (14.7 mmHg) so real trans-vascular pressure is actually very low at 0.3 mmHg
So why aren’t we using them?
Apart from lack of education or understanding, the unwillingness to spend extra time inserting, trouble shooting and yest sometimes getting frustrated with them
- Not available on all current ventilators: lame excuse but remember it was developed in the 70s before most ICU ventilators had graphics even, yes it is easier to have the catheter attached and graphs displayed on the ventilator but it can be connected to regular ICU monitor (need to convert mmHg to cmH2O, hard to compare to the other ventilator waveforms)
- Expensive: ok maybe you have a point there but compared to other expenses in ICU it actually is not that expensive
- No good evidence for improved outcomes: i hear you, there are some evidence not very strong but there is actually not much good research still so lets do some work. Remember they said that about prone position and steroids for ARDS right ?
- There are other options or technologies for measurements: good, we need multi-modal monitoring (look at the blog multi-modal monitoring)
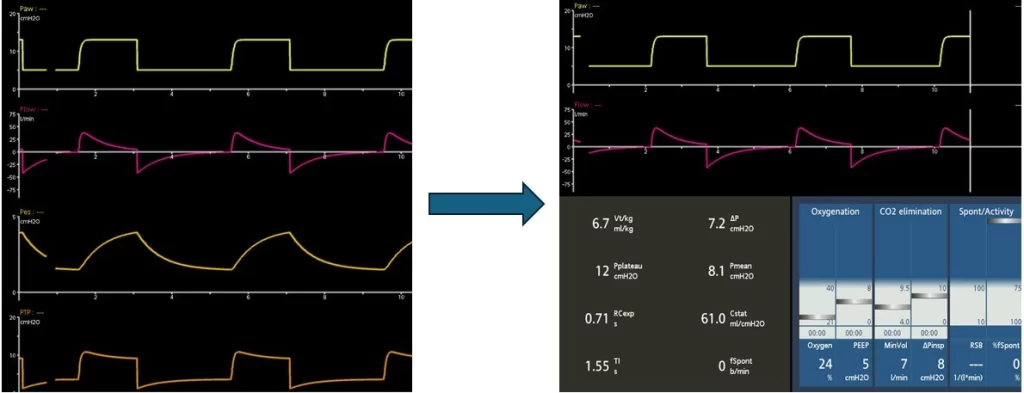
Having a problem with it or don’t want to deal with it ? No problem, Easy
Change the screen and pretend it is not there
The change in end-expiratory lung volume is determined by the elastic properties of the LUNG and the size of the PEEP change (DEELV = Clung x DPEEP). On the basis of this finding, we have developed a non-invasive, esophageal pressure free method for separating lung and chest wall mechanics. For a full assessment of the lung P/V curve, only a two PEEP step manouvre is required, where DEELV is determined between PEEP levels. Consequently, lung compliance can be determined as DEELV/DPEEP. From the equation of the best-fit curve of the lung P/V curve optimal PEEP, i.e., the PEEP level with lowest (least injurious) transpulmonary driving pressure can be determined. Also, transpulmonary driving pressure of any combination of PEEP and tidal volume (VT) can be calculated, which gives clinical decision support whether a cerain setting of PEEP/VT is possible without risking dangerous transpulmonary driving pressure or plateau pressure.
A two PEEP step measurement procedure only takes about three minutes. (Stenqvist, Crit Care 2024, Grivans Physiol Meas 2022, Persson Br J Anaesth 2022. These studies are all open access).
The reason why esophageal pressure measurements (PES) are not used is that it is unprecise, cumbersome and expensive. In addition, there are contradictory ways to interpret results: PAW – absolute PES (Talmor – Loring) and the elastance method (Gattinoni). These two methods have shown incompatible results when selecting PEEP (Gulati, CCM 2013) . In addition, a large RCT showed that the Talmor Loring method did not reduce mortality (Beitler JAMA 2019).
The change in end-expiratory lung volume is determined by the elastic properties of the LUNG and the size of the PEEP change (DEELV = Clung x DPEEP)[1]. Based on this finding, we have developed a non-invasive, esophageal pressure free method for separating lung and chest wall mechanics. For a full assessment of the lung P/V curve, only a two PEEP step manouvre is required, where DEELV is determined between PEEP levels. Consequently, lung compliance can be determined as DEELV/DPEEP. From the equation of the best-fit curve of the lung P/V curve optimal PEEP, i.e., the PEEP level with lowest (least injurious) transpulmonary driving pressure can be determined. Also, transpulmonary driving pressure of any combination of PEEP and tidal volume (VT) can be calculated, which gives clinical decision support whether a cerain setting of PEEP/VT is possible without risking dangerous transpulmonary driving pressure or plateau pressure.
A two PEEP step measurement procedure only takes about three minutes. (Stenqvist, Crit Care 2024, Grivans Physiol Meas 2022, Persson Br J Anaesth 2022 [1-3]. These studies are all open access).
The reason why esophageal pressure measurements (PES) are not used is that it is unprecise, cumbersome and expensive. In addition, there are contradictory ways to interpret results: PAW – absolute PES (Talmor – Loring)[4] and the elastance method (Gattinoni)[5]. These two methods have shown incompatible results when selecting PEEP (Gulati, CCM 2013) [6]. In addition, a large RCT showed that the Talmor Loring method did not reduce mortality (Beitler JAMA 2019[7]).
1. Stenqvist O: Transpulmonary pressure monitoring in critically ill patients: pros and cons-correction of description of the non-invasive PEEP-step method for separation of lung and chest wall mechanics. Critical care 2024, 28(1):355.
2. Grivans C, Stenqvist O: Gas distribution by EIT during PEEP inflation: PEEP response and optimal PEEP with lowest trans-pulmonary driving pressure can be determined without esophageal pressure during a rapid PEEP trial in patients with acute respiratory failure. Physiological measurement 2022, 43(11).
3. Persson P, Stenqvist O: Protective positive end-expiratory pressure and tidal volume adapted to lung compliance determined by a rapid positive end-expiratory pressure-step procedure in the operating theatre: a post hoc analysis. British journal of anaesthesia 2022, 128(4):e284-e286.
4. Talmor D, Sarge T, Malhotra A, O’Donnell CR, Ritz R, Lisbon A, Novack V, Loring SH: Mechanical ventilation guided by esophageal pressure in acute lung injury. The New England journal of medicine 2008, 359(20):2095-2104.
5. Gattinoni L, Chiumello D, Carlesso E, Valenza F: Bench-to-bedside review: chest wall elastance in acute lung injury/acute respiratory distress syndrome patients. Critical care 2004, 8(5):350-355.
6. Gulati G, Novero A, Loring SH, Talmor D: Pleural pressure and optimal positive end-expiratory pressure based on esophageal pressure versus chest wall elastance: incompatible results*. Critical care medicine 2013, 41(8):1951-1957.
7. Beitler JR, Sarge T, Banner-Goodspeed VM, Gong MN, Cook D, Novack V, Loring SH, Talmor D, Group EP-S: Effect of Titrating Positive End-Expiratory Pressure (PEEP) With an Esophageal Pressure-Guided Strategy vs an Empirical High PEEP-Fio2 Strategy on Death and Days Free From Mechanical Ventilation Among Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA : the journal of the American Medical Association 2019.